How Hype Nest Global helped a mid-size hospital eliminate manual workflows, reclaim 1,200 staff hours every month, and cut per-patient administrative costs by 64%—without replacing a single team member.
Executive Summary
AI workflow automation in healthcare is no longer a future investment — it is an operational necessity. This case study documents how Hype Nest Global deployed a purpose-built AI automation system for a 340-bed hospital operations team, integrating directly with their existing EHR platform with zero disruption to clinical workflows.
Three headline results achieved within 90 days:
- 1,200 staff hours reclaimed per month — equivalent to 7.5 full-time employees
- 64% reduction in per-patient administrative cost (from $47.20 to $16.99)
- 91% reduction in scheduling errors across three departments
No staff were replaced. No new software was forced on frontline teams. The system worked inside the tools the hospital already used — and delivered measurable ROI by Month 4.
According to McKinsey, healthcare providers that deploy AI in administrative workflows reduce operational costs by 30–40% within the first year. This case study shows what that looks like in practice.
The Operational Challenge: What Staff Were Doing Manually
Before engaging Hype Nest Global, the hospital’s operations team was spending the majority of their working day on tasks that required zero clinical judgment — pure data movement, copy-paste coordination, and manual report generation.
The operations director’s estimate: 40+ hours lost per day to manual admin.
Specifically, staff were spending time on:
- Manually cross-referencing nurse availability against shift requirements in a separate Excel file
- Copy-pasting patient data between EHR modules and the scheduling system
- Pulling compliance reports from three disconnected platforms and combining them by hand
- Re-entering insurance pre-authorization data that had already been captured at intake
- Making manual follow-up calls to coordinate lab results and discharge paperwork
The financial cost was significant. The human cost was worse.
Two experienced coordinators had resigned in the quarter before the project began. Both cited administrative overload as a primary reason. A third was actively looking to leave. The team described their daily experience as “feeding the system instead of doing actual work.”
This is the hidden cost of manual hospital operations — not just money, but the people who can no longer bear doing it.
AI Solution Architecture: Agent + EHR Integration
Hype Nest Global designed a three-layer AI automation stack tailored specifically to hospital operations. The entire system was built to integrate with the hospital’s existing EHR — no rip-and-replace, no new interfaces for frontline staff to learn.
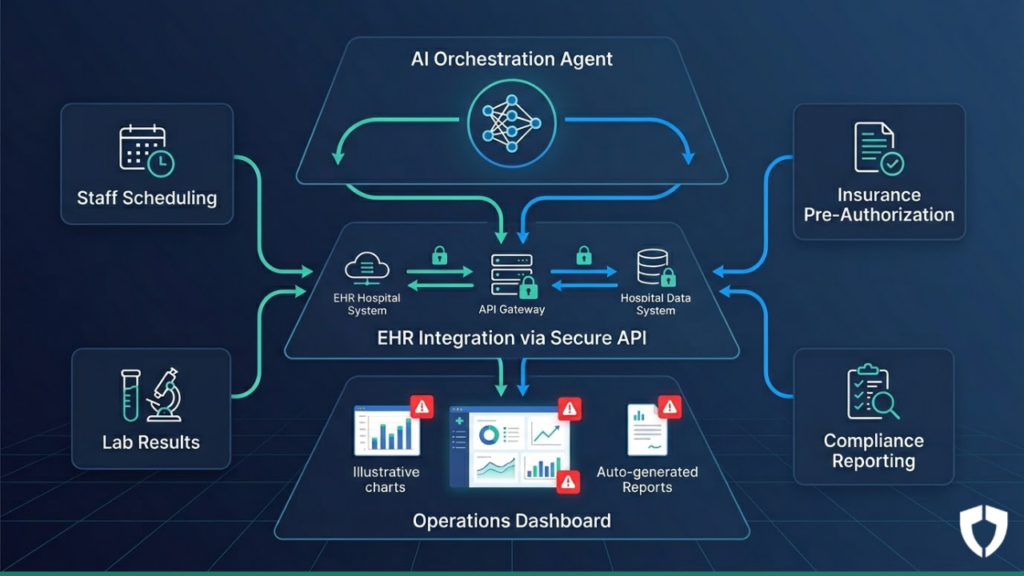
Layer 1 — AI Orchestration Agent
A central AI agent monitors triggers across all operational systems in real time. When a condition is met — a shift gap appears, a pre-authorization request arrives, a lab result is flagged — the agent initiates the correct automated workflow instantly, without human prompting.
Layer 2 — EHR Integration via Secure API
The system connects to the EHR using a HIPAA-compliant read/write API layer. Data moves directly between systems, eliminating manual copy-paste entirely. Every transfer is logged and auditable.
Layer 3 — Operations Dashboard
Staff no longer generate reports manually. The dashboard auto-produces daily operational summaries, surfaces anomalies, and presents only the decisions that genuinely require a human. Everything else is handled automatically.
Key integrations built:
- EHR ↔ Staff Scheduling Module (bi-directional sync)
- Insurance Portal ↔ Pre-Authorization Workflow (automated submission and tracking)
- Lab System ↔ Discharge Coordination Agent (result-triggered alerts)
- Compliance Module ↔ Auto-Report Generator (scheduled and on-demand)
Before vs. After: Hospital Operations Workflow Comparison
| Workflow | Before Automation | After Automation | Time Saved |
|---|---|---|---|
| Nurse shift scheduling | 3.5 hrs/day, manual | AI-generated in 4 minutes | ~3.4 hrs/day |
| Insurance pre-authorization | 22 min per case | Auto-submitted in 90 seconds | ~18 min per case |
| Compliance report generation | 6 hrs/week, 2 staff | Auto-generated, reviewed in 20 min | ~5.7 hrs/week |
| Lab result follow-up | Manual calls + notes | Automated alerts + EHR update | ~2 hrs/day |
| Patient discharge admin | 45 min per discharge | 12 min with AI-assisted checklist | ~33 min per discharge |
| Daily operations summary | 1.5 hrs each morning | Ready automatically at 6:00 AM | ~1.5 hrs/day |
Every workflow in the table above was previously owned by a human. After automation, each one runs on a trigger — and a human only steps in when an exception requires judgment.
Results: Hours Saved, Cost Reduction, and Staff Experience
Operational Efficiency
Hospital operations AI automation delivered across every metric tracked:
- 1,200 staff hours reclaimed per month across scheduling, reporting, and coordination
- Per-patient administrative cost dropped from $47.20 to $16.99 — a 64% reduction
- Pre-authorization approval cycle cut from 3.2 days to 11 hours
- Scheduling errors reduced by 91%, virtually eliminating understaffed shifts
Financial Impact
- Annualised administrative savings of approximately $380,000
- Full ROI achieved by Month 4 of deployment
- Total implementation cost recovered within the first operating year
Staff Experience
This is where the results surprised the operations director most.
In a follow-up survey conducted 60 days post-deployment:
- 87% of operations staff reported feeling significantly less stressed during their shifts
- Coordinator turnover dropped to zero in the quarter following deployment
- Three staff members who had been considering leaving chose to stay
- The team’s own description of the change: “We’re doing actual work now instead of feeding the system”
AI healthcare staff scheduling and workflow automation did not eliminate jobs. It eliminated the parts of jobs that were making people leave — and that distinction matters when healthcare faces a chronic staffing crisis.
Implementation Timeline: Weeks 1 Through 12
Weeks 1–2: Discovery and Workflow Audit
The Hype Nest Global team embedded with hospital operations to map every manual workflow from observation — not assumption. Every task was timed. Every data source was identified. Every integration dependency was documented before a single line of code was written.
Weeks 3–4: Architecture Design and EHR Integration Planning
The AI agent architecture was scoped and documented. API access to the EHR was tested in a sandboxed environment. HIPAA compliance requirements were reviewed and baked into the data handling design from day one — not added afterwards.
Weeks 5–7: Build and Integration
Core automations were built and connected: scheduling sync, pre-authorization workflow, and lab result alerts. Operations staff were briefed clearly on what would change and, just as importantly, what would not.
Weeks 8–9: Parallel Testing
Every automated workflow ran alongside the existing manual process simultaneously. Staff validated outputs against what they would have produced manually. Edge cases were identified and resolved. No workflow went live until it matched or exceeded the accuracy of the human process.
Weeks 10–11: Phased Go-Live
Automations were activated department by department — never all at once. A dedicated Hype Nest Global contact was available daily. Every issue raised was resolved within 24 hours.
Week 12: Handoff, Training, and Dashboard Activation
The operations team received full documentation, a custom SOPs guide, and a half-day training session covering the dashboard and exception-handling process. Weekly check-in calls ran for 30 days post-handoff.
Key Lessons and What We Would Do Differently
What worked well
Starting with high-volume, low-complexity workflows first — scheduling and report generation — built trust quickly and delivered visible wins before tackling more complex integrations. When staff saw the system work on familiar tasks, resistance to the later, more significant changes dropped sharply.
Involving frontline coordinators — not just directors — in the workflow audit produced materially better results. The coordinators knew exactly where time was being lost. The director knew what the problems were in aggregate. Both perspectives were essential.
Parallel testing eliminated the fear of errors. Staff did not have to trust the system on faith — they watched it prove itself against their own work before it went live.
What we would do differently
Start the EHR API access approval process on Day 1, not Week 3. Hospital IT security reviews take longer than anticipated. This delayed the integration build by five days and compressed the testing window unnecessarily.
Introduce the exception dashboard earlier — in Week 2, not Week 10. Without seeing it, staff felt they were losing visibility into their own operations. Showing the dashboard concept early, even as a wireframe, would have significantly reduced anxiety throughout the project.
Build a structured internal communication plan. We relied on the operations director to brief the team. A formal communication approach — owned by the project, not delegated — would have reduced informal resistance and accelerated adoption.
Is Your Hospital Operations Team Ready for AI Workflow Automation?
The hospital in this case study is not exceptional. Most mid-size hospital operations teams carry a hidden administrative burden that healthcare AI ROI analysis consistently underestimates — because no one has ever measured it properly.
The first step is a clear picture of where the hours are actually going.
Is your hospital operations team losing hours to manual workflows? Book a free 30-minute AI Workflow Audit with our team.
We will map your three highest-volume manual workflows, estimate the staff hours and cost they carry each month, and show you exactly what an automation solution would look like for your specific environment.
No pitch. No commitment. A clear, honest picture of what is possible.
Book Your Free AI Workflow Audit – Click Here